Parina Anand, Product Manager, at ARMMAN, brings to life the voices that shaped the journey of development of the chatbot that is bridging the gaps in access to healthcare for women.

“I will ask my questions here because no one would insult me at least,” shared Mahira*, when asked if she would use ARMMAN’s pregnancy and infancy care chatbot. “Here, I can ask a question any number of times.” She was alluding to the dismissal she had likely experienced at the hands of the doctors and nurses, for asking too many or basic questions.
India’s public health system is overburdened. A multi-country study published in BMJ Open found that the average doctor-patient consultation time in India is just 3.8 minutes, leaving little space for explanation, follow-up, or questions. As a result, advice is often brief and can come across as curt or unempathetic, failing to satisfy even the most confident and curious women.
When we set out to build a chatbot within Kilkari, the world’s largest maternal messaging programme, which has reached more than 75 million women and their children, our goal was to respond to a demand we were seeing everywhere: women wanting answers to their specific health queries. In a pilot on WhatsApp-based messaging with about 500 women in Jharkhand and Haryana in 2023, 67% engaged in two-way communication and 20% asked at least one question despite no active encouragement. In every subsequent user research study, we found a growing number of women turning to YouTube and Instagram for pregnancy-related queries. It was clear: women have questions, and they are actively seeking answers. What they lack are trustworthy sources. We had spent months in user research and internal discussions, trying to define the goal of this chatbot. And then Mahira captured it succinctly in one sentence: it would fill the gap between advice from doctors and incorrect advice from family members or social media, while giving women a safe space.
Curiosity as the Real Driver of Technology Adoption
Over six months in 2025, across the slums of Delhi and Mumbai and the villages of Jharkhand and Bihar, our design researchers uncovered fascinating insights into what we collectively termed information-seeking behaviours among pregnant women and mothers of infants. We found that factors traditionally considered determinants of success for technology-enabled public-sector tools like education, phone ownership, income, had surprisingly little to do with digital savviness. The real determinant was curiosity. In maternal and child health, curiosity is shaped by deeper factors: exposure (through work or migration), number of pregnancies, complications in previous pregnancies, and to some extent, age. Literacy, which is often independent of formal education, showed little correlation.
“My previous two pregnancies resulted in miscarriage. I really don’t want it to happen this time as well, so I ask questions on YouTube about do’s and don’ts,” Seema*, 28, told us. She had never attended school and could neither read nor write. During a live onboarding to the chatbot in a public hospital setting, she immediately asked a question on the service, without any nudging. She used WhatsApp’s voice note feature to ask her questions in Hindi. When she received the response in both text and audio, she downloaded the audio and listened to it instantly.
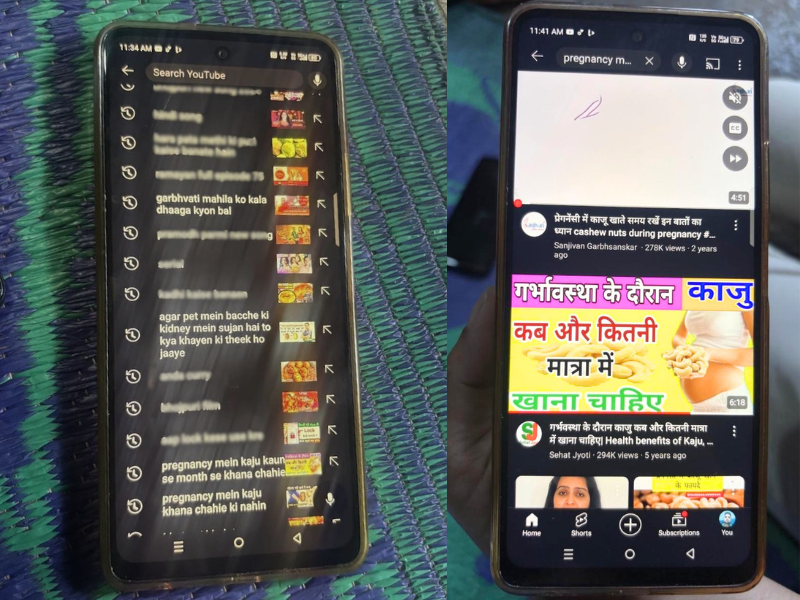
We saw this behaviour repeatedly. Curious women figure out how to use technology. They use voice search on YouTube, scan images in video result pages to judge relevance, compare multiple sources to decide what to trust, even without being able to read.
When access does not translate into use of digital tools
“So this is like ChatGPT?” asked Rutuja*, 27, graduate, in her first pregnancy.
She had used ChatGPT before but only to interpret medical reports before doctor visits. When asked if she had ever asked other questions, she said no, she had never felt the need. She was one of only three women out of ten who did not ask a single question during the chatbot session, even when nudged with scenarios and prompts. When prompted with scenarios like post-delivery child care, she said, “I am completely dependent on my mother for all that; I will do as she tells me.” For taboo questions, which are often cited as a major use case for faceless chatbots, she said she had friends she could ask.In the presence of multiple trusted information sources and a smooth, low-risk pregnancy, we found that digital information-seeking remained low, even among highly educated women with access and exposure. Seema and Rutuja show us how wide this spectrum really is, and how important it is to challenge our assumptions about who will be a “power user” of chatbots. While it was clear that Seema would be the more active user of the two, this is not a concern, she is the one who needs it most. But what about users who need the chatbot yet stand at the passive end of the spectrum?

We found that women with multiple pregnancies and no major complications, and sometimes minor risk factors like prior C-sections, displayed very little information-seeking behaviour. In the Indian context, this is often compounded by patriarchal family structures, where women have limited agency and are rarely encouraged to ask questions. Despite multiple nudges and scenario-based prompts, Sarita*, 27, a third-time pregnant woman, studied till 8th grade, told us she felt “shy” and had “never asked questions.” If we were not able to convince her in-person, it is hard to believe that positioning or nudges alone could overcome this barrier.
Role of household influencers
We also found that this behaviour changes significantly when couples migrate to metropolitan cities like Mumbai. Even when little else changes, the influence of extended family reduces, and the husband’s involvement increases, especially when it is just the two of them navigating pregnancy and childcare. In Mumbai, where our chatbot is currently being piloted, we frequently see husbands actively engaging with doctors, asking questions themselves, and encouraging their wives to do the same. While we are yet to conduct focused studies on expectant fathers, hospital visits during our research have shown encouraging signs.

Another critical stakeholder for a pregnancy care chatbot is the mother of the pregnant woman. In India, women often spend a significant part of pregnancy and the postpartum period in their maternal home. This makes mothers central to care, especially when husbands live elsewhere. Unlike more patriarchal setups that prioritise only the child’s well-being, mothers often care deeply about the health of the woman herself.
“We will also ask questions. We want to know what and when we should be feeding our daughter,” one mother of a pregnant woman told us. Another gently encouraged her hesitant daughter: “Go ahead and ask the question.”
Designing for trust, dignity, and agency
At ARMMAN, our approach is to share gender-transformative content and advice that is culturally sensitive, but also aspires toward a better, more equitable normal.
While many questions remain unanswered, ones we hope to explore through continued research, experiments, and learning from users themselves, we are optimistic. A pregnancy and infancy care chatbot responds to a real and growing need for trustworthy, judgment-free information. When designed with deep attention to context and lived realities, it can become a reliable extension of care within India’s public health infrastructure.